Treating high blood pressure without medication
Renal Denervation in Switzerland
Minimally invasive. Effective. Lasting blood pressure reduction.
Renal denervation is a minimally invasive and innovative treatment for hypertension. Performed via catheterisation, this procedure reduces the activity of renal sympathetic nerves responsible for elevated blood pressure. It is particularly indicated for patients whose hypertension responds poorly or is resistant to medication, or in cases of intolerance or bothersome side effects. Recent clinical studies (SPYRAL HTN-ON MED, RADIANCE-HTN TRIO) confirm its efficacy and safety.
Why choose renal denervation?
Minimally invasive procedure
outpatient under general anaesthesia, no scar
Performed by interventional radiologist and cardiologist
under image guidance
Proven efficacy
supported by numerous recent scientific studies
Covered by basic health insurance
LAMal in Switzerland
Multidisciplinary care
including radiology, nephrology, cardiology and general medicine
Hypertension is a very common condition in our ageing society. It is estimated that approximately 30 to 45% of adults are affected, and its prevalence increases significantly with age, exceeding 60% in people over 60. Often asymptomatic, it can nevertheless lead to serious cardiovascular complications in the long term, particularly when diagnosis is delayed or treatment is inadequate. Under the influence of factors such as excess weight, sedentary lifestyle and excessive salt intake, blood pressure rises gradually, imposing constant stress on the arteries and heart. This chronic elevation increases the risk of cardiac, renal and cerebrovascular diseases, and requires early management to prevent complications.
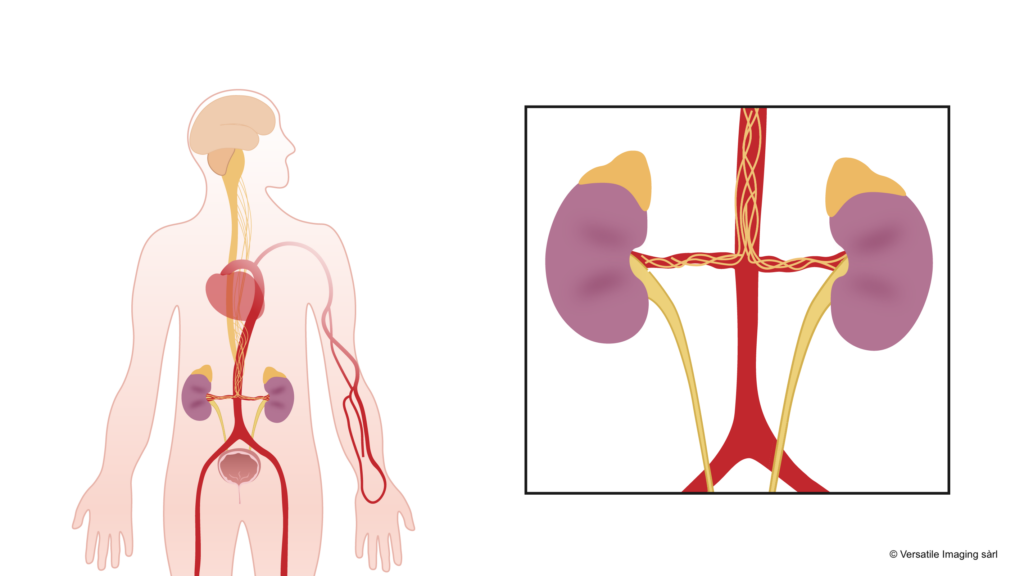
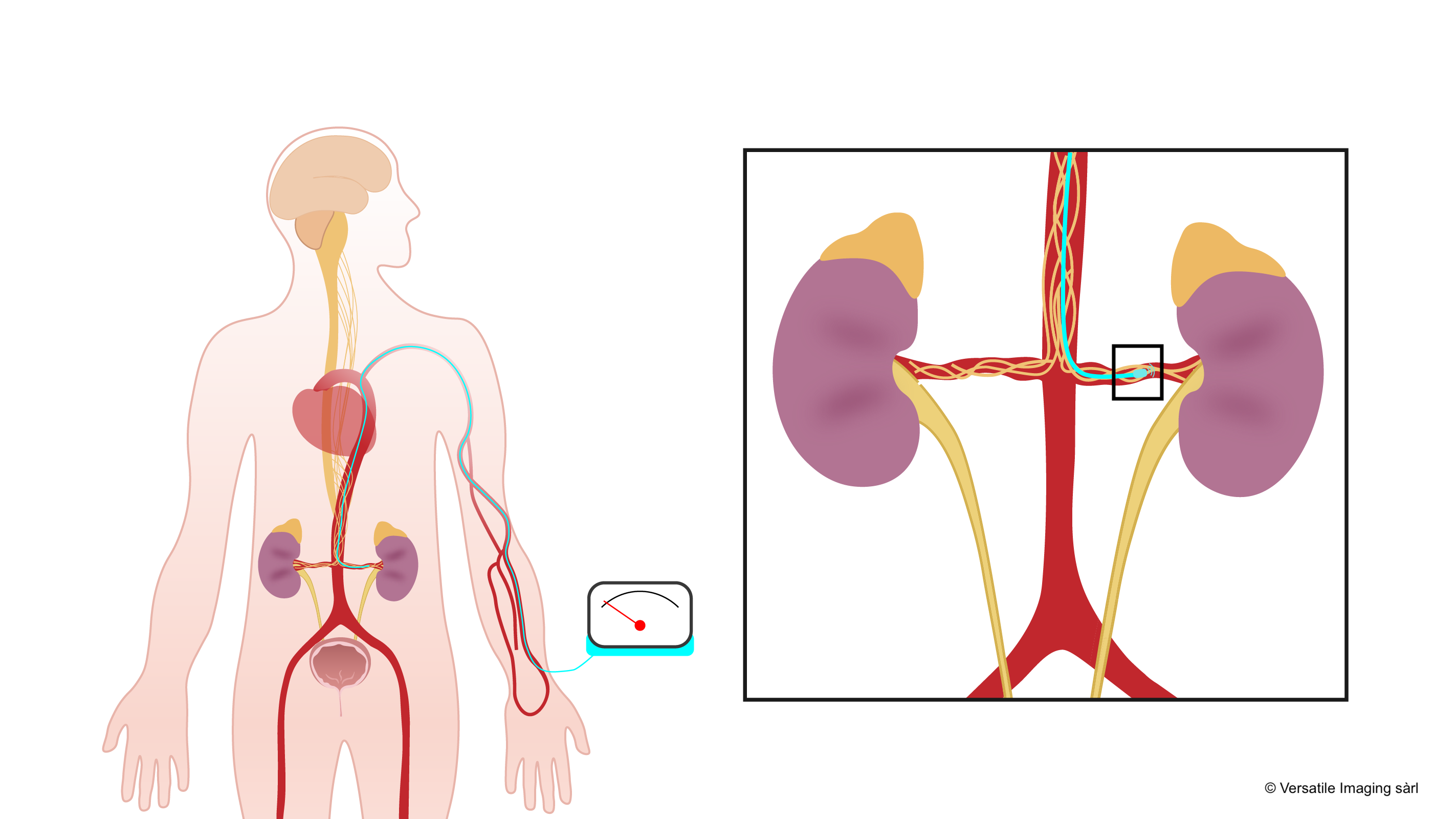
The role of the kidney in blood pressure
The kidney acts as a "pressure regulator" for our body. It manages the amount of water and salt we retain or eliminate, which directly influences the volume of circulating blood and therefore blood pressure. The kidney also produces a substance called "renin", which triggers a chain of reactions (the renin-angiotensin-aldosterone system) that can raise blood pressure when it is too low. However, if this mechanism goes into overdrive (for example due to a kidney problem or overproduction of renin), blood pressure can become too high. In turn, the kidneys can suffer from this excessive pressure, creating a vicious cycle where the problem worsens.
The kidney and the nervous system communicate closely to maintain balanced blood pressure. Nerves called "sympathetic nerves" control, for example, the degree of constriction of the kidney's blood vessels and the release of renin. When they become overactive, they amplify vessel constriction and renin production, driving up blood pressure. Conversely, when these nerves are less stimulated, blood pressure can decrease. The kidney also sends signals to the brain to inform it of the state of blood pressure and blood composition, showing how important this constant dialogue is for the proper functioning of the entire system.

How is blood pressure measured?
There are several ways to measure blood pressure. The most common is office measurement: the healthcare professional uses an inflatable cuff around the arm, often taking several readings, to ensure reliable values. Home blood pressure monitoring (HBPM) allows tracking blood pressure in the usual daily environment, without the stress associated with the "white coat" effect. Finally, ambulatory blood pressure monitoring (ABPM) involves wearing a small device that automatically records values throughout the day and night. Using these different methods, a more accurate picture of blood pressure is obtained, and treatment can be better adjusted if necessary.
What are the recommended blood pressure targets?
Blood pressure is generally considered normal when it is below 140/90 mmHg. Below these values, the risks of complications (such as strokes or heart attacks) are significantly reduced. For some people, particularly those already suffering from cardiovascular disease, diabetes or kidney problems, doctors may recommend even lower targets, such as 130/80 mmHg. The idea is to adapt targets to each individual situation, in order to best prevent the risks associated with hypertension.
Resistant hypertension
Hypertension (high blood pressure) is one of the most common chronic diseases worldwide. It affects approximately 1.3 billion people and is the leading risk factor for stroke, heart attack, heart failure and chronic kidney disease. Hypertension is defined as systolic blood pressure ≥ 140 mmHg and/or diastolic blood pressure ≥ 90 mmHg.
Resistant hypertension is defined as blood pressure that remains above target despite treatment with at least three antihypertensive medications of different classes, including a diuretic, at optimal doses. This affects approximately 10 to 15% of hypertensive patients, representing millions of people worldwide.
Risks of uncontrolled hypertension
Cardiovascular risks
Uncontrolled hypertension significantly increases the risk of stroke, heart attack, heart failure and peripheral arterial disease. Each 20 mmHg increase in systolic pressure doubles cardiovascular risk.
Target organ damage
Chronic hypertension progressively damages the kidneys (renal failure), eyes (hypertensive retinopathy), brain (vascular dementia) and heart (left ventricular hypertrophy). This damage is often silent and irreversible.
Hypertension is often called the "silent killer" because it usually causes no symptoms before significant damage to vital organs has occurred.
Standard treatment of hypertension
The treatment of hypertension relies on several complementary approaches:
- Lifestyle modifications (salt reduction, physical activity, weight loss, limiting alcohol);
- Antihypertensive medications;
- Renal denervation for medication-resistant cases.
Drug treatments
Drug therapy is the cornerstone of hypertension management. Several classes of medications may be prescribed, often in combination.
ACE inhibitors and ARBs
These medications act on the renin-angiotensin-aldosterone system to lower blood pressure. They are often prescribed as first-line therapy. Possible side effects: dry cough (ACE inhibitors), hyperkalaemia, functional renal impairment.
Calcium channel blockers
Calcium channel blockers relax the smooth muscles of blood vessels, thereby reducing arterial resistance. Possible side effects: ankle oedema, flushing, palpitations.
Diuretics
Diuretics promote the elimination of sodium and water by the kidneys, reducing blood volume and thus blood pressure. Possible side effects: hypokalaemia, dehydration, muscle cramps, gout.
Beta-blockers
Beta-blockers slow the heart rate and reduce the force of heart contraction. Possible side effects: fatigue, bradycardia, sleep disturbances, impotence.

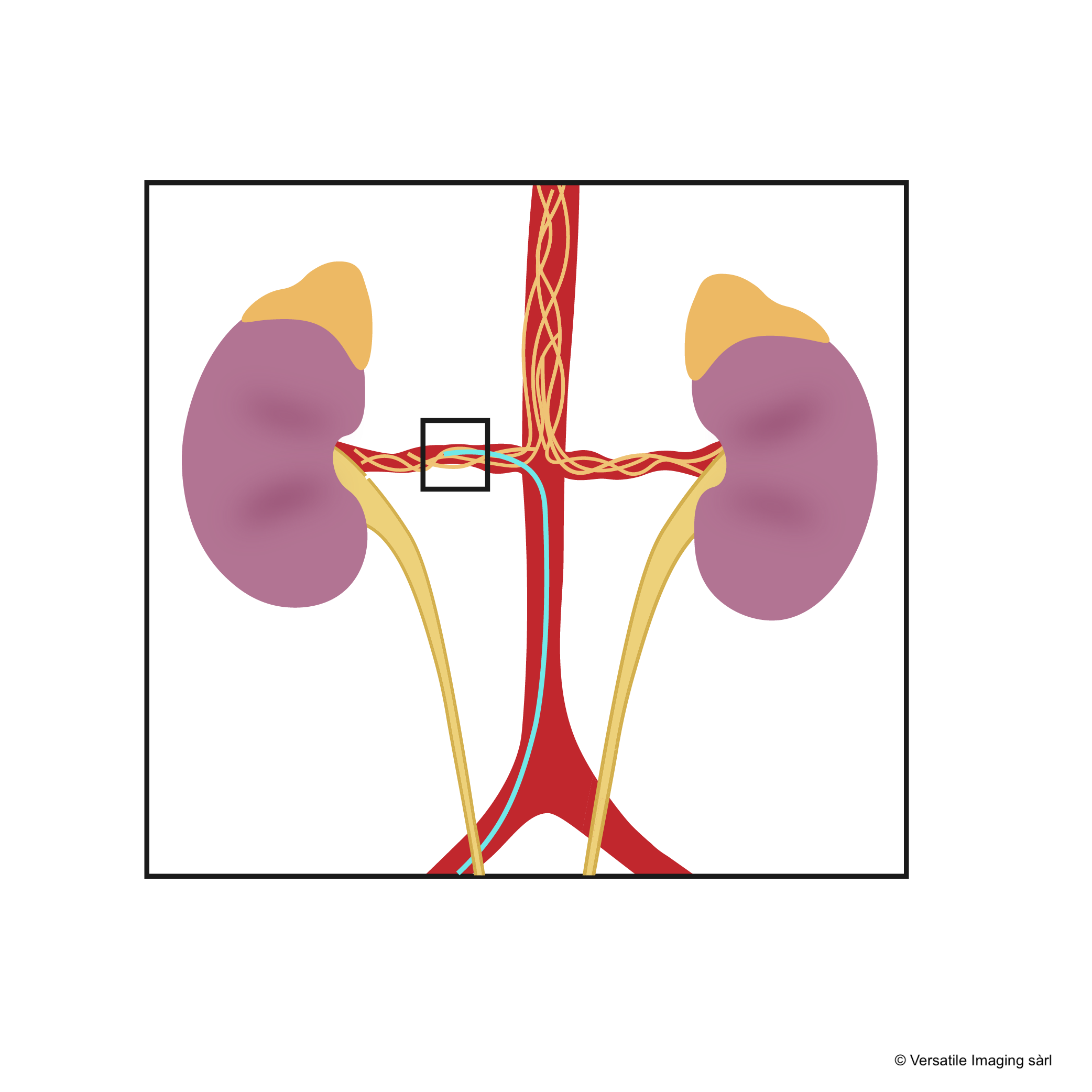
Renal denervation procedure
Principle
Renal denervation is a minimally invasive interventional radiology procedure that aims to reduce the activity of the renal sympathetic nervous system. The sympathetic nerves running along the renal arteries play a key role in blood pressure regulation. When overactive, they contribute to hypertension by increasing sodium retention, stimulating renin secretion and reducing renal blood flow. The procedure involves inserting a catheter through the femoral artery (at the groin) into the renal arteries, then delivering energy (radiofrequency or ultrasound) to modulate these nerves.
Pre-procedural consultation
During your consultation with the interventional radiologist, a comprehensive assessment will be carried out to determine whether you are a suitable candidate for renal denervation. This assessment includes: a history of your hypertension and treatments tried, a 24-hour ambulatory blood pressure monitoring (ABPM), blood tests (renal function, electrolytes), and renal artery imaging (CT angiography or MR angiography) to verify the vascular anatomy and exclude renal artery stenosis. It is essential to rule out secondary causes of hypertension (renal artery stenosis, phaeochromocytoma, hyperaldosteronism) before the procedure.
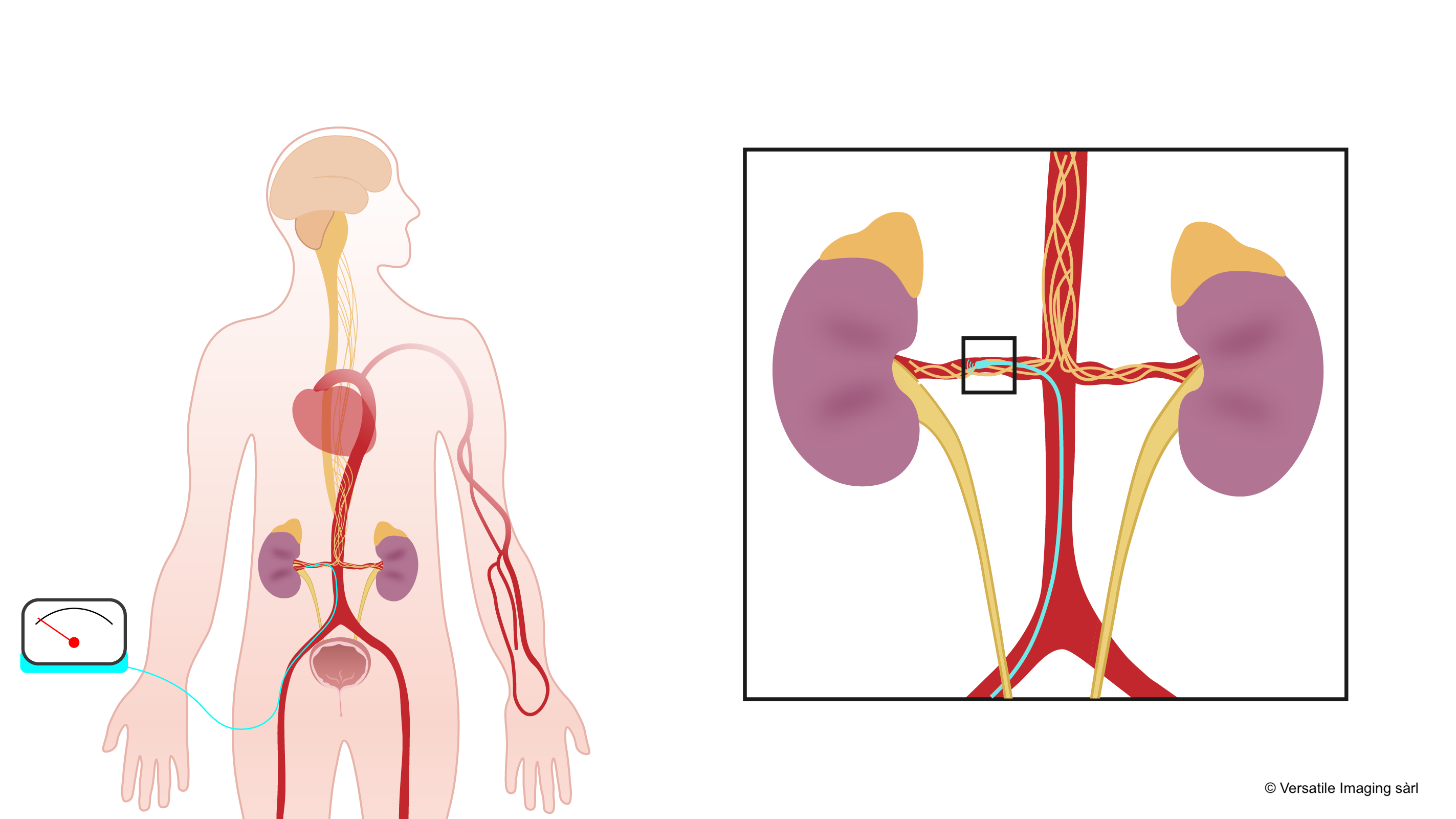
The procedure
The procedure is performed on an outpatient basis or during a short hospital stay, in an interventional radiology suite, under local anaesthesia and light sedation.
The procedure takes place in a sterile environment. You will be positioned on the radiology table. Medical staff will set up an IV line and monitor your blood pressure and heart rate.
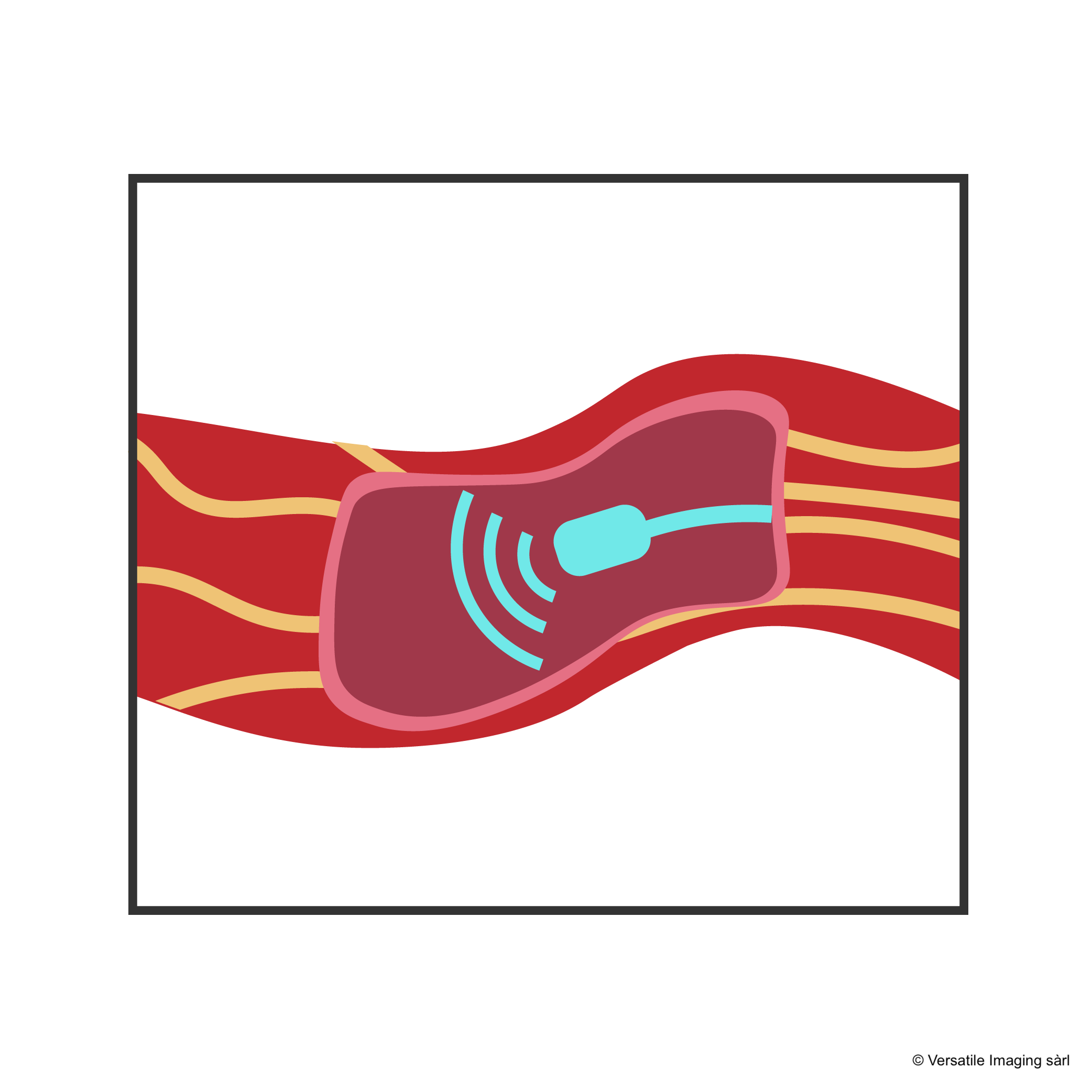
Renal denervation involves 5 main steps
Procedure duration
Renal denervation takes approximately 45 minutes to 1.5 hours, depending on the renal artery anatomy. Both renal arteries (right and left) are treated during the same procedure.
Post-procedure follow-up
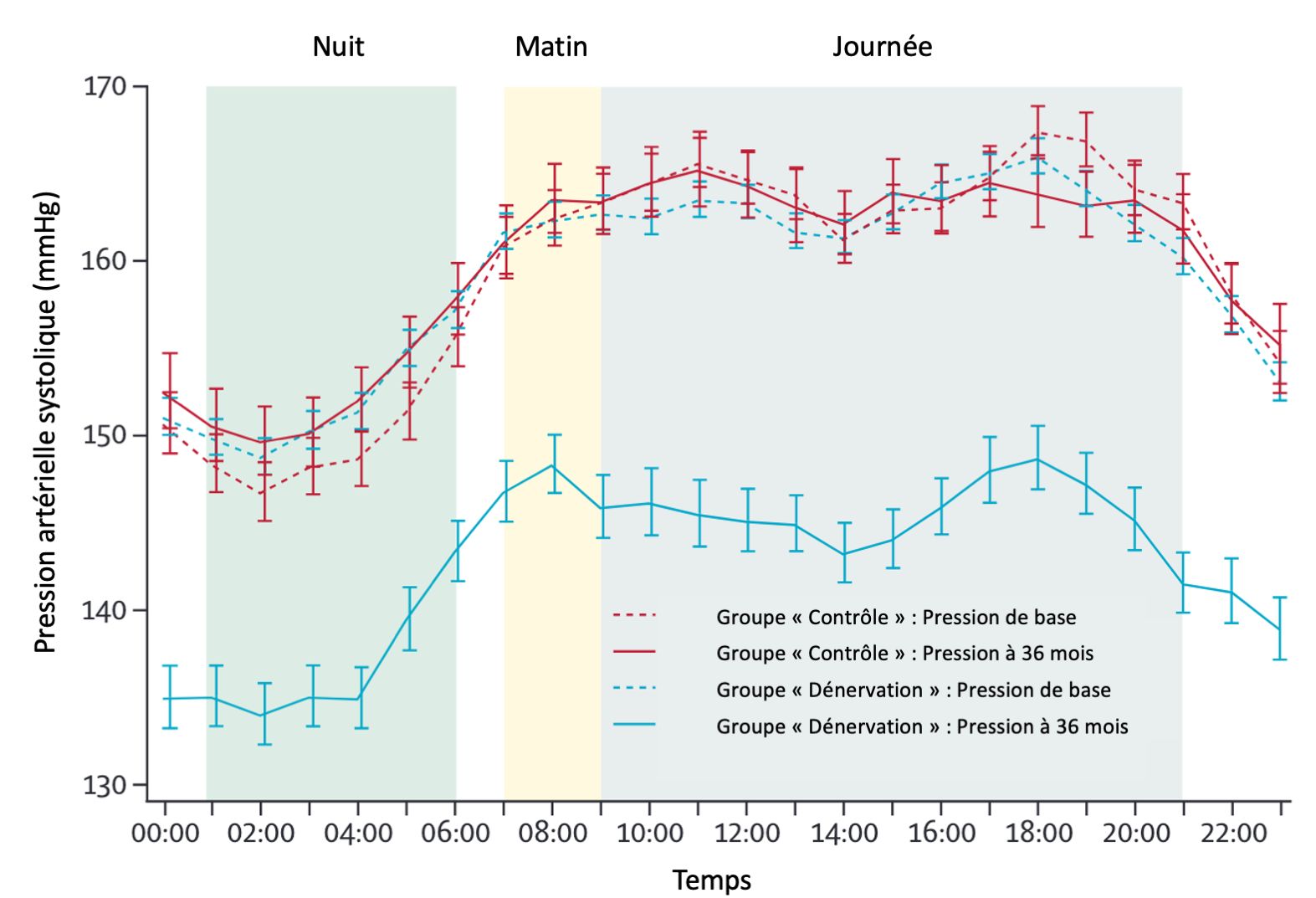
After the procedure, you will be monitored for several hours before returning home. Blood pressure will be regularly monitored during follow-up consultations at 1, 3 and 6 months, then annually. The blood pressure reduction is progressive, with maximum effect typically achieved between 3 and 6 months. Medication will be maintained initially and then adjusted (potentially reduced) by your doctor based on blood pressure trends.
Renal denervation versus medication alone
| Criterion | Medication alone | Renal denervation |
|---|---|---|
| Efficacy in resistant cases | Limited (uncontrolled BP despite ≥3 medications) | Significant additional BP reduction |
| Adherence | Problematic (50% of patients do not take medications correctly) | Permanent effect, independent of adherence |
| Side effects | Frequent (fatigue, impotence, cough, cramps, oedema) | Rare and transient (mild pain at puncture site) |
| Treatment duration | Lifelong, daily | Single procedure, lasting effect |
| Hospitalisation | No (daily oral intake) | Outpatient or short hospitalisation |
| Medication reduction | No (often additional medications required) | Possible (reduction in number of medications) |
Scientific studies
Renal denervation is supported by high-level randomised clinical trials that have demonstrated its efficacy and safety in the treatment of resistant hypertension.
SPYRAL HTN-ON MED (2020)
The SPYRAL HTN-ON MED study is a randomised, sham-controlled, multicentre trial evaluating the efficacy of radiofrequency renal denervation in addition to antihypertensive medication.
The 80 enrolled patients were receiving 1 to 3 antihypertensive medications at stable doses. The primary endpoint was the change in 24-hour ambulatory blood pressure at 6 months.
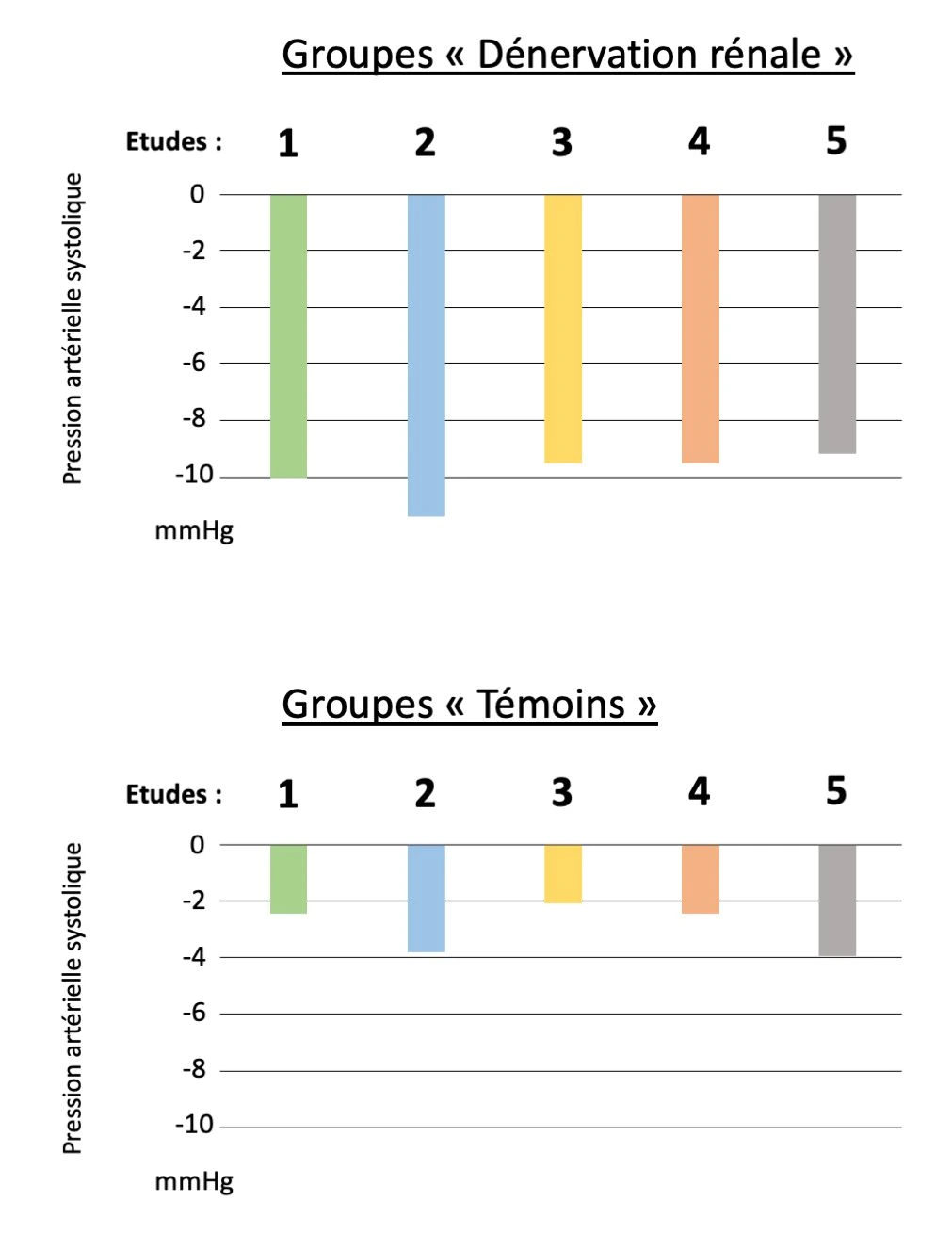
Results showed a significant systolic blood pressure reduction of -7.0 mmHg in office measurement and -3.9 mmHg in 24-hour ambulatory measurement in the denervation group compared to the control group.
RADIANCE-HTN TRIO (2022)
The RADIANCE-HTN TRIO study is a randomised, sham-controlled, multicentre trial evaluating endovascular ultrasound renal denervation in patients with confirmed resistant hypertension.
After a treatment standardisation phase (fixed triple combination: amlodipine, valsartan, hydrochlorothiazide), 136 patients whose blood pressure remained uncontrolled were randomised between ultrasound renal denervation or sham procedure.
At 2 months, the reduction in daytime ambulatory systolic blood pressure was -8.0 mmHg in the denervation group versus -3.0 mmHg in the control group, a difference of -4.5 mmHg in favour of denervation (p = 0.022).
RADIANCE II (2023)
The RADIANCE II study is the largest sham-controlled randomised trial evaluating endovascular ultrasound renal denervation. It enrolled 224 patients with uncontrolled hypertension despite 0 to 2 antihypertensive medications across 61 centres in 6 countries. This FDA pivotal trial confirmed the superiority of ultrasound renal denervation over sham procedure, with significant reduction in daytime ambulatory systolic blood pressure at 2 months.
The reduction in daytime ambulatory systolic blood pressure was -7.9 mmHg in the denervation group versus -1.8 mmHg in the control group, a difference of -6.3 mmHg (p < 0.001).
Read the RADIANCE II study (JACC) →Your specialist

Dr Nicolas Villard
Interventional Radiologist
Dr Nicolas Villard is a Swiss physician specialising in interventional radiology. Expert in endovascular techniques, he offers renal denervation to patients in Western Switzerland suffering from resistant hypertension.
With his expertise in interventional radiology and endovascular procedures, he masters the most advanced techniques to ensure optimal results while minimising risks for the patient.
He practises in Lausanne and Geneva, in close collaboration with cardiologists and nephrologists in the region. Consultations are available in French, English and German.
Consultation and treatment locations
Clinique Générale Beaulieu
Chemin de Beau-Soleil 20, 1206 Geneva
List of specialists involved in this treatment in Western Switzerland →
Book an appointment
For a consultation, contact Dr Villard's office.
Please send your recent results (cardiology/nephrology reports, ABPM, blood tests, renal artery imaging) to the office.
Book an appointment online with Dr N. Villard
Select a time slot online for a consultation in Geneva or Lausanne.
Frequently asked questions about renal denervation
Note: It is essential to consult your interventional radiology specialist for personalised information tailored to your health status.
Angiotensin II receptor blockers (ARBs / sartans) — losartan, valsartan, candesartan, irbesartan, olmesartan: dizziness, hyperkalaemia, muscle pain, digestive problems, and rarely angioedema.
Calcium channel blockers — amlodipine, nifedipine, lercanidipine, felodipine: ankle swelling (very common with amlodipine), hot flushes, headaches, palpitations, gingivitis.
Beta-blockers — bisoprolol, metoprolol, nebivolol, atenolol, carvedilol: chronic fatigue, bradycardia, cold extremities, sleep disturbances and nightmares, erectile dysfunction, weight gain, asthma worsening.
Thiazide diuretics — hydrochlorothiazide, indapamide, chlorthalidone: hypokalaemia (cramps, muscle weakness), hyponatraemia, hyperuricaemia and gout attacks, dehydration, dizziness, skin photosensitivity, increased cholesterol and blood sugar.
Aldosterone antagonists — spironolactone, eplerenone: hyperkalaemia, painful gynaecomastia in men (spironolactone), menstrual disorders in women, fatigue.
Alpha-blockers — doxazosin, prazosin: orthostatic hypotension (fall risk), dizziness, drowsiness, nasal congestion, reflex tachycardia.
Given these sometimes debilitating side effects, renal denervation offers an attractive alternative: a single procedure, with no daily medication, that effectively and durably lowers blood pressure by acting on the very cause of hypertension.
Their most common side effects include:
• Persistent dry cough — the most characteristic side effect, affecting up to 10% of patients. This irritating cough, often nocturnal, only resolves when the medication is stopped.
• Angioedema — sudden swelling of the face, lips, tongue or throat. Rare but potentially serious, requiring emergency consultation.
• Hyperkalaemia — excess potassium in the blood, which can cause heart rhythm disturbances.
• Dizziness and hypotension — especially at the start of treatment or when increasing the dose.
• Fatigue and taste disturbance.
• Acute kidney failure — in cases of bilateral renal artery stenosis (contraindication).
If you experience these side effects, talk to your doctor: a treatment adjustment (changing molecule, dose modification) may be considered. But the most lasting solution is renal denervation: it lowers blood pressure in a single procedure, without daily medication and without the risk of cough or angioedema.
Their side effects include:
• Dizziness and lightheadedness — especially at the start of treatment.
• Hyperkalaemia — elevated blood potassium, increased risk with kidney impairment or combination with other medications.
• Muscle and joint pain.
• Digestive problems — nausea, diarrhoea, abdominal pain.
• Headaches and fatigue.
• Angioedema — rare, but possible even in patients who switched from an ACE inhibitor due to cough.
• Kidney impairment — in cases of bilateral renal artery stenosis.
Although generally better tolerated than ACE inhibitors, ARBs still require lifelong daily intake. If you experience side effects, your doctor can adjust the treatment or consider an alternative. The most effective solution remains renal denervation: a single procedure that durably reduces blood pressure, potentially freeing the patient from this long-term medication.
Their common side effects include:
• Ankle and leg swelling — the most common and bothersome side effect, affecting up to 20–30% of patients on amlodipine. Ankles swell, sometimes very visibly, and this oedema does not respond to diuretics.
• Hot flushes and facial flushing — a sensation of heat in the face and neck.
• Headaches — frequent, especially at the start of treatment.
• Palpitations and tachycardia — the heart beats faster in response to vasodilation.
• Gingivitis and gum overgrowth — gum swelling, especially with long-term nifedipine.
• Constipation — particularly with verapamil (Isoptin®).
Ankle swelling on amlodipine is one of the leading causes of treatment discontinuation. If you are bothered by these side effects, consult your doctor to evaluate a treatment adjustment. Better still, renal denervation avoids this problem entirely: by lowering blood pressure through a single procedure, it can enable reduction or discontinuation of these medications and their bothersome side effects.
Their side effects are numerous and often poorly tolerated:
• Chronic fatigue and low energy — the most frequently reported side effect. Patients feel "slowed down", lacking motivation and endurance.
• Bradycardia — excessively slow heart rate, causing dizziness and faintness.
• Cold extremities — permanently cold hands and feet, worsening of Raynaud's syndrome.
• Sleep disturbances — insomnia, nightmares, non-restorative sleep (especially with lipophilic beta-blockers such as metoprolol).
• Erectile dysfunction and decreased libido — a frequent side effect rarely mentioned spontaneously by patients (see the dedicated question below).
• Weight gain — on average 1 to 3 kg, due to metabolic slowing.
• Bronchospasm — worsening of asthma and COPD.
• Depression and low mood.
• Masking of hypoglycaemia in diabetic patients.
Beta-blockers have a considerable impact on quality of life. If you experience side effects, your doctor can adjust the treatment (change of molecule, dose reduction). But the best alternative remains renal denervation: it effectively lowers blood pressure in a single session, without fatigue, without sleep disturbance, without impact on libido — and without daily tablets.
Their side effects include:
• Hypokalaemia — potassium loss causing muscle cramps, weakness, fatigue and potentially heart rhythm disturbances.
• Hyponatraemia — low blood sodium, which can cause confusion, nausea, and even seizures in elderly patients.
• Hyperuricaemia and gout attacks — increased uric acid, triggering painful joint attacks.
• Dehydration — especially in summer or in elderly patients, with risk of faintness and falls.
• Dizziness and orthostatic hypotension — risk of falling when standing up.
• Skin photosensitivity — increased sun sensitivity, risk of severe sunburn (particularly hydrochlorothiazide, associated with increased skin cancer risk with prolonged exposure).
• Increased blood sugar and cholesterol — potential worsening of diabetes and dyslipidaemia.
• Erectile dysfunction — an often underestimated effect.
• Frequent urination — constraining in daily life.
If you experience bothersome side effects, talk to your doctor about adjusting your treatment. But above all, renal denervation can reduce the need for diuretics by lowering blood pressure directly at its source — in a single procedure, effectively and durably.
Their side effects include:
• Gynaecomastia — breast development in men, sometimes painful. This is the most feared side effect of spironolactone, affecting up to 10% of treated men. It is related to the anti-androgenic effect of the molecule (see the dedicated question below).
• Hyperkalaemia — excess blood potassium, potentially dangerous for the heart, requiring regular blood monitoring.
• Menstrual disorders — irregular periods, spotting, amenorrhoea in women.
• Decreased libido and sexual dysfunction — in both men and women.
• Fatigue and drowsiness.
• Digestive problems — nausea, diarrhoea.
Eplerenone (Inspra®) causes less gynaecomastia than spironolactone, but it is more expensive and less potent. If these side effects affect you, your doctor can adjust the treatment (switching to eplerenone, dose adjustment). But for patients with resistant hypertension, renal denervation offers the best alternative: a single procedure that lowers blood pressure effectively, without gynaecomastia, without hormonal disturbances and without additional medication.
Their side effects include:
• Orthostatic hypotension — sudden drop in blood pressure when standing, with high risk of falls. This is the main danger, especially in elderly patients. Can cause syncope and injury.
• Dizziness and lightheadedness — very common, especially with the first dose ("first-dose effect").
• Drowsiness and fatigue.
• Nasal congestion — permanently blocked nose.
• Reflex tachycardia — increased heart rate.
• Oedema.
• Retrograde ejaculation — in some men.
The risk of falls from orthostatic hypotension is a major concern, particularly in elderly patients. If you are affected, your doctor can adjust the dosage or consider another medication class. Better still, renal denervation does not cause orthostatic hypotension: it lowers blood pressure in a physiological and stable manner, in a single procedure, without the blood pressure fluctuations associated with alpha-blockers.
Erectile dysfunction and libido problems:
• Beta-blockers (Concor®, Beloc ZOK®, Tenormin®) — the most frequently implicated class. Erectile dysfunction affects up to 5–10% of treated men. The mechanism is twofold: reduced cardiac output and blockade of adrenergic receptors involved in erection. Nebivolol (Nebilet®) appears to cause fewer erectile problems than other beta-blockers.
• Thiazide diuretics (Esidrex®, Hygroton®) — cause erectile dysfunction through reduced blood volume and electrolyte imbalance.
• Spironolactone (Aldactone®) — direct anti-androgenic effect, reducing testosterone. Causes decreased libido in both men and women.
• Alpha-blockers (Cardura®) — may cause retrograde ejaculation.
Gynaecomastia (breast development in men):
Spironolactone (Aldactone®) is the main culprit. Its anti-androgenic effect blocks testosterone action and promotes oestrogen effects, causing breast tissue development in men. This affects up to 10% of treated patients. Breasts may become tender, painful, and visibly enlarged. This effect is dose-dependent and generally reversible upon discontinuation, but sometimes only partially.
Impact on quality of life:
These sexual and hormonal problems are often kept silent by patients out of embarrassment, yet they are a major cause of unsupervised treatment discontinuation — with potentially serious consequences for cardiovascular health. Do not hesitate to discuss this with your doctor: a treatment adjustment (changing molecule, dose modification) can often improve the situation.
But the best solution remains renal denervation: it has no effect on sexual function, libido or hormonal balance. By reducing blood pressure in a single procedure, it can enable reduction or discontinuation of the medications causing these problems — restoring patients' quality of life without compromising blood pressure control.
Specialists involved in this treatment in Western Switzerland

